What is ApoB and Why Does It Matter More Than LDL?

Key Highlights
Apolipoprotein B (ApoB) is increasingly recognized as a more accurate predictor of cardiovascular disease than traditional LDL cholesterol, especially when ApoB and LDL-C are discordant
Understand the key differences between ApoB and LDL cholesterol and their roles in your heart health.
Learn how ApoB testing offers other insights into your heart disease risk than a standard cholesterol panel.
Explore the factors that influence your ApoB levels, including diet, genetics, and metabolic health.
Discover effective ways to monitor and lower your ApoB for better cardiovascular outcomes.
Introduction
When your doctor mentions high cholesterol, your mind probably jumps to LDL the familiar "bad" cholesterol. But what if there's a more precise way to understand your cardiovascular risk? That's where Apolipoprotein B (ApoB) comes in. While a traditional lipid panel tells part of the story, your ApoB level can give a clearer, more actionable, picture. This article explains why ApoB has emerged as a critical marker for heart health and how it can guide more effective prevention and treatment.
ApoB and LDL Cholesterol the Basics
Understanding cholesterol means looking past the simple "good" and "bad" framing. ApoB and LDL cholesterol are related but measure different things one counts particles, the other measures the cargo those particles carry.
What Is Apolipoprotein B (ApoB)?
Apolipoprotein B is the structural protein found on the surface of every atherogenic lipoprotein including LDL, VLDL, IDL, and Lp(a). Each of these particles carries exactly one ApoB molecule, which means measuring ApoB gives you a direct count of the particles capable of driving plaque formation in your arteries.
Think of ApoB as the "license plate" or “VIN” on every cholesterol-carrying vehicle that can damage your arterial walls. The higher your ApoB, the more of these vehicles are circulating in your bloodstream and the greater your risk of cardiovascular disease.
Understanding LDL Cholesterol
LDL cholesterol low-density lipoprotein cholesterol is often called "bad" cholesterol because excess LDL contributes to atherosclerosis, the plaque buildup that narrows arteries and drives heart attacks and strokes. But here's the nuance: a standard LDL test measures the amount of cholesterol carried inside LDL particles, not the number of particles themselves.
That distinction matters more than most patients realize.
How ApoB Differs from LDL Cholesterol
Two people can have identical LDL cholesterol numbers but very different cardiovascular risk profiles. Why? Because LDL particles vary in size and density. Someone with many small, dense LDL particles can have a "normal" LDL cholesterol reading while carrying a dangerous number of atherogenic particles each one capable of penetrating the arterial wall.
ApoB cuts through this ambiguity by counting every atherogenic particle directly.
Feature
| Feature | LDL Cholesterol | Apolipoprotein B (ApoB) |
|---|---|---|
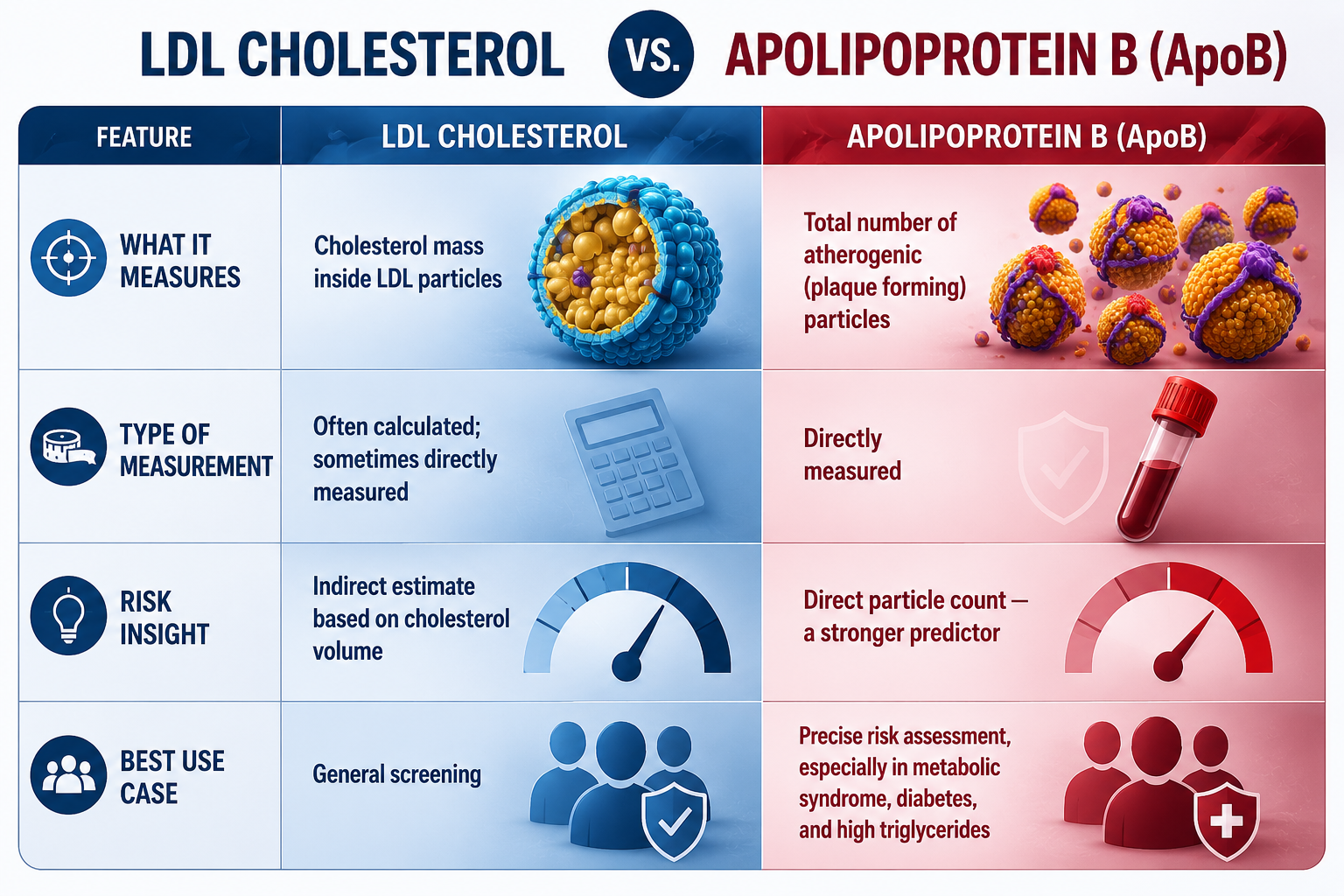
| What it measures | Cholesterol mass inside LDL particles | Total number of atherogenic (plaque-forming) particles |
| Type of measurement | Often calculated; sometimes directly measured | Directly measured |
| Risk insight | Indirect estimate based on cholesterol volume | Direct particle count — stronger predictor |
| Best use case | General screening | Precise risk assessment (metabolic syndrome, diabetes, high triglycerides) |
risk, Particularly Why ApoB Is a Superior Indicator of Cardiovascular Risk
Mounting evidence shows that ApoB outperforms LDL cholesterol as a predictor of heart disease risk particularly in patients whose lipid profiles don't fit the textbook pattern.
The Scientific Evidenceburden, including
Large prospective studies and meta-analyses have consistently found that ApoB levels are more strongly associated with future heart attacks and cardiovascular events than LDL cholesterol or non-HDL cholesterol. A landmark 2021 study in JAMA Cardiology analyzing data from nearly 400,000 individuals found that ApoB captured cardiovascular risk more accurately than either LDL-C or non-HDL-C, and that once you account for ApoB, those other markers add little additional predictive value.
The reason is mechanistic: atherosclerosis is driven by the number of ApoB-containing particles that infiltrate the arterial wall, not the total cholesterol they happen to be carrying that day.
Why Cardiologists and Lipid Specialists Are Shifting to ApoB
Leading lipidologists increasingly recommend ApoB testing because it offers:
A direct particle count. No estimation, no calculation just the number of atherogenic particles in your blood.
Better consistency. ApoB testing is highly standardized across labs, and unlike a calculated LDL value, it isn't distorted by high triglycerides or recent meals.
Sharper risk stratification. ApoB identifies high-risk patients who would be missed by LDL testing alone — particularly those with metabolic syndrome, type 2 diabetes, or insulin resistance.
Medical Guidelines Are Shifting
Major guidelines have started to reflect this evidence. The European Society of Cardiology and European Atherosclerosis Society (ESC/EAS) guidelines explicitly recognize ApoB as a preferred risk marker, particularly in patients with high triglycerides, diabetes, obesity, or metabolic syndrome. The National Lipid Association in the US has also endorsed ApoB as a clinically useful measure for refining cardiovascular risk assessment, and the AHA/ACC guidelines include ApoB as a "risk-enhancing factor."
Common recommendations now include:
Using ApoB instead of (or alongside) LDL-C, especially when triglycerides are elevated.
Considering ApoB in patients with a strong family history of premature heart disease.
Setting specific ApoB targets for high-risk patients to guide therapy.
The Role of ApoB in Cholesterol Testing
How ApoB Reflects Atherogenic Particle Number
Because every atherogenic lipoprotein carries one ApoB protein, your ApoB level is essentially a census of the particles that can damage your arteries. A higher count means more opportunities for particles to penetrate the arterial wall and trigger plaque formation — regardless of how much cholesterol each one is carrying.
This is why two patients with identical LDL cholesterol can have very different ApoB levels, and very different real-world risk.
ApoB Testing vs. a Traditional Lipid Panel
A standard lipid panel reports total cholesterol, HDL, LDL, and triglycerides. The LDL value is often calculated using either the Friedewald or Martin-Hopkins equation rather than measured directly. Both can be reasonably accurate, but they lose precision when triglycerides are high or when LDL is very low exactly the situations where accurate risk assessment matters most.
ApoB testing, by contrast, directly measures the concentration of ApoB protein in your blood. The method is automated, highly standardized, and consistent across labs.
Advantages of ApoB testing:
Direct measurement rather than estimation.
Standardized methodology that produces reliable results across laboratories.
Captures total atherogenic burden including risk from VLDL and remnant particles, not just LDL.
Common Misconceptions About ApoB and LDL
A few myths worth clearing up:
"Normal LDL means I'm safe." Not necessarily. You can have normal LDL cholesterol with elevated ApoB a discordance that hides real risk.
"ApoB is just another cholesterol test." It's not. ApoB measures something fundamentally different: particle number, not cholesterol content.
"My standard panel is enough." For many patients it is but for anyone with metabolic syndrome, diabetes, high triglycerides, or premature family history of heart disease, ApoB often provides decision-changing information.
How to Test for ApoB in the United States
ApoB testing is widely available in the US through major reference labs including Quest Diagnostics and LabCorp, as well as most hospital lab systems. The process is straightforward:
Discuss ApoB testing with your healthcare provider particularly if you have metabolic syndrome, diabetes, high triglycerides, or a family history of premature heart disease.
Your provider orders the test, typically alongside or in place of a standard lipid panel.
Visit a participating lab for a simple blood draw.
ApoB testing alone does not require fasting. However, if it's ordered with a lipid panel, your provider may still ask you to fast follow their specific instructions.
How to Interpret ApoB Results
ApoB results are reported in milligrams per deciliter (mg/dL). Lower is generally better, but optimal targets depend on your individual cardiovascular risk profile.
Optimal: Below 60 mg/dL
Moderate risk: 70 mg/dL
Elevated risk: Above 90 mg/dL
For patients with established cardiovascular disease or very high risk, lipid specialists often target ApoB levels well below 65 mg/dL, and below 50–60 mg/dL for the highest-risk patients. Your provider will interpret your number in the context of your age, blood pressure, family history, diabetes status, and other risk factors.
When ApoB Provides More Accurate Information Than LDL
ApoB is especially valuable in situations where LDL cholesterol can mislead:
Metabolic syndrome and insulin resistance. These patients often have many small, dense LDL particles. Each carries less cholesterol, so total LDL-C may look normal but particle count (ApoB) is high.
Type 2 diabetes. Similar pattern: discordance between LDL-C and particle number is common.
High triglycerides. Calculated LDL becomes unreliable, while ApoB remains accurate.
Patients on statin therapy. ApoB often reveals residual risk that LDL-C alone misses.
In all of these cases, ApoB confirms whether the true atherogenic burden matches what the LDL number suggests and frequently it doesn't.
Conclusion
Understanding ApoB is one of the most important shifts in modern cardiovascular risk assessment. Where LDL cholesterol gives a partial view, ApoB provides a direct count of the particles that actually drive atherosclerosis. The science supports it, leading guidelines increasingly recommend it, and patients with metabolic syndrome, diabetes, or strong family history of heart disease have the most to gain from getting tested.
If you're curious about your own ApoB level and what it means for your heart health, our team is here to help. Book a free consultation with Mechanic MD to get personalized insights into your cardiovascular risk and a clear plan for what to do next.
Frequently Asked Questions
Does having normal LDL mean my ApoB is also normal? Not necessarily. You can have a normal LDL cholesterol level but elevated ApoB a situation called discordance. This is especially common in people with metabolic syndrome, insulin resistance, or type 2 diabetes, and it can hide significant cardiovascular risk that a standard cholesterol test would miss.
Why could high ApoB mean more risk than high LDL? Atherosclerosis is driven by the number of atherogenic particles entering the arterial wall, not the total cholesterol those particles carry. Because each atherogenic particle carries one ApoB protein, a high ApoB level directly signals a high number of plaque-forming particles making it a stronger predictor of heart disease risk than LDL cholesterol alone.
Is ApoB testing standardized and reliable compared to LDL cholesterol testing? Yes. ApoB testing is automated and highly standardized across laboratories. Standard LDL cholesterol values, by contrast, are often calculated rather than directly measured, which can introduce inaccuracies especially when triglycerides are high or LDL is very low. This makes ApoB a more dependable measure in many clinical scenarios.
Should I get an ApoB test if my standard lipid panel looks fine? If you have metabolic syndrome, type 2 diabetes, insulin resistance, high triglycerides, a strong family history of premature heart disease, or known cardiovascular disease, ApoB testing is worth discussing with your provider even if your LDL looks normal. For low-risk individuals with a clean lipid panel and no other risk factors, the additional value is smaller.